{kind=link}
下颌正中管的锥形束CT三维重建
[刘成军1  , 艾毅龙
, 艾毅龙2 ]
, 艾毅龙]
|
|


作者简介:刘成军,副主任医师,硕士,Email:liuchengjun@126.com
目的 通过锥形束CT(CBCT)扫描对下颌正中管的存在与否、走向及其与周围组织的三维关系进行评估及测量,为颏下区手术的安全提供保障。方法 对100例患者的CBCT图像进行三维重建并测量。测量项目包括Mandibular Icisive Canal (MIC)的存在与否,MIC垂直向和水平向直径,MIC在下颌管起始点,第一前磨牙对应点,尖牙对应点,切牙对应点至牙根尖、下颌骨颊侧壁、舌侧壁、下颌下缘以及牙槽嵴顶的垂直距离。结果 100例CBCT中百分百可见MIC。MIC与颊侧骨板和舌侧骨板平均距离分别为3.52 ± 0.54 mm 和5.37 ± 0.25 mm,与下颌骨下缘、牙根尖和牙槽嵴顶的平均距离为10.44 ± 0.61、10.57 ± 0.76及20.21 ± 0.83 mm。MIC到下颌骨下缘的距离男性为10.70 ± 0.43 mm,女性为10.17 ± 0.63 mm, P<0.05,差异具有统计学意义。结论 MIC在CBCT中检出率高且走向各异。
Objective To find out the existence of Mandibular Incisive Canal (MIC) through CBCT scanning and measure its 3D relationship with the surrounding tissue, so as to provide protection for the operation in submental area.Methods CBCT images of 100 patients were measured and three dimensionally reconstructed. The measurement include following items, the existence of the MIC; vertical and horizontal diameter of MIC; vertical distance from MIC to the mandibular buccal and lingual wall; to the root apex, to the inferior border of mandible and alveolar crest in corresponding points (the mandibular first premolar, canine and incisor).Results the MIC was 100% visible in CBCT. The mean distance between MIC and buccal bone plate and lingual bone plate was 3.52 ± 0.54 mm and 5.37 ± 0.25 mm. The average distance from the inferior border of the mandible, the apex of the root and the crest of the alveolar bone was 10.44 ± 0.61 mm、10.57 ± 0.76 mm and 20.21 ± 0.83 mm relatively. The distance from MIC to the inferior border of the mandible in male was 10.70 ± 0.43 mm and 10.17 ± 0.63 mm in female, P<0.05.Conclusion The detection rate of MIC is high and there are many variations. It was suggested that the location and size of the MIC should be checked in CBCT in each patient before operation, which is helpful to avoid surgical complications in submental area.
下颌切牙神经是下牙槽神经的末端分支, 支配下颌切牙及尖牙的感觉。过去较多学者认为该神经游走于骨髓之间, 没有骨性的管道, 常规摄影无法检测[1]。随着科学技术的进步, 越来越多的证据证明下颌正中管(MIC)的存在, 其直径较小, 骨化程度较弱, 管里为神经血管束, 由颏孔起始向近中行走至下颌骨前部, 正好位于下前牙根下方[2]。对需要在此区域进行手术的患者, 如种植体的植入, 下颌颏部取骨, 颏成形术等, 下颌正中管的检出具有重大的意义。如果在术前忽视下颌正中管, 可能导致术后的神经麻木, 水肿, 血肿, 种植体骨整合的失败, 牙髓神经敏感改变等[3]。本研究应用CBCT三维重建技术, 对广东佛山人各年龄组的下颌骨颏孔间区域进行了系统性的影像学检查。
于2015年1月-2015年12月间在佛山市口腔医院放射科拍摄过下颌骨CBCT的所有患者中分别随机抽取男女患者资料各50例, 共100例, 左侧下颌骨区及右侧下颌骨区分开计算, 即总样本为200个。纳入标准:年龄在18岁到55岁之间; 颏孔间区无牙齿缺失, 牙齿轻度拥挤以下, 未有龋齿、根尖周炎、牙周炎等; 既往无颏下区手术、外伤等。排除标准:牙齿中度或中度以上拥挤; 有全身系统性疾病者; 有颌骨畸形、外伤、肿瘤病变等。
按年龄将患者分为3组, 分为18~30岁年龄组, 31~44岁年龄组及45~55岁年龄组。
所有受检者均采用CBCT(ProMax3D, Planmeca OY公司, 芬兰)按以下技术进行全扫描。体位:坐位, 头部用支架固定, 眶耳平面与地面平行, 颏部用颏托固定。由机器发出的正中垂直光束与受检者面部中线对齐, 水平光束与眶平面平行。扫描条件:扫描视野为110~130 mm, 扫描电压为96 kV, 辐射电流12 mA, 体素0.2 mm。扫描后所有扫描图像数据均被传入Planmeca自带数据处理中心进行三维重建。
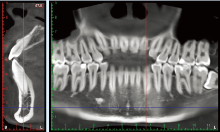
所有的数据均由同一位受过训练的口腔外科医生进行测量, 两周后再测量一次, 取两次的平均值。在CBCT上评估下颌正中管从开始到结束的走向。根据下颌管的走向, 在全景截面上找出下颌管起始点, 及第一前磨牙、尖牙、切牙和结束点对应的MIC, 在这些位置上截取其矢状面, 在矢状面上测量MIC垂直向和水平向的直径, MIC到下颌骨颊舌侧骨板的水平距离, MIC到牙根尖, 下颌骨边缘和牙槽嵴顶的距离(图1)。如果下颌正中管在某个牙位对应的位置已经消失, 则在数据上标记为0。
使用SPSS 12.0对不同性别间的测量数据进行两样本t检验进行统计学分析, 对不同年龄组间的测量数据进行LSD单因素方差分析。
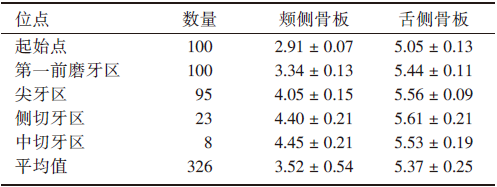
在CBCT检测中, 所有的MIC都是由颏孔位置开始, 在第一前磨牙对应处100%能观察到MIC, 在尖牙区域也有95%能观察到, 但仅有23%在切牙区仍能观察到。MIC的直径从开始到结束越来越小(表1)。典型下颌正中管见图1。只有1%的样本在下颌中部的时候还有一个比较大的直径( > 1 mm)。MIC与颊侧骨板和舌侧骨板平均距离分别为3.52 ± 0.54 mm 和5.37 ± 0.25 mm, 说明其更靠近颊侧骨板(表2)。与下颌骨下缘、牙根尖和牙槽嵴顶的平均距离为10.44 ± 0.61、10.57 ± 0.76及20.21 ± 0.83 mm, 在所有的位点中MIC到牙槽嵴顶的距离都大于到下颌骨下缘的距离(表3)。这些数据中不同性别间有差异的仅有MIC到下颌骨下缘的距离, 男性为10.70 ± 0.43 mm, 女性为10.17 ± 0.63 mm, 女性MIC更靠近下颌骨下缘, P< 0.05(表4)。不同年龄分组中MIC到下颌骨下缘的距离没有统计学差异, P > 0.05(表5)。
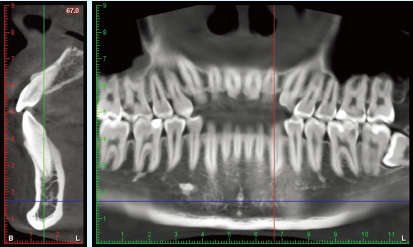 | 图1 MIC在不同位点垂直向和水平向的直径Figure 1 Mandibular Incisive Canal |
| 表1 典型下颌正中管 Table 1 Vertical and horizontal diameters of MIC at different sites ( |
| 表2 MIC在不同位点与颊侧和舌侧骨板的垂直距离 Table 2 the vertical distance between MIC and buccal or lingual cortical at different sites( |
| 表3 MIC在不同位点与下颌骨下缘、牙根尖和牙槽嵴顶的垂直距离 Table 3 Vertical distance of MIC to the lower margin of mandible, root apex and alveolar crest at different sites( |
| 表4 男女MIC与三维方向平均距离的对比 Table 4 Comparison of distance in MIC between male and female three dimensionally( |
| 表5 不同年龄分组MIC三维方向平均距离的对比 Table 5 Comparison of distance of MIC in different age groups three dimensionally( |
MIC为下前牙及周围粘膜提供神经支配。然而, 由于MIC的骨性结构并不明显, 直径也比下颌管小, 所以经常被忽略。MIC最早是在尸体解剖中发现的[4], 有学者指出在尸体解剖中所有双侧下颌骨均能找到MIC, 但是, 在常规的全景片中很难观察到MIC。Jacobs等[5]专家报道其观察的全景片中仅有15%能观察到MIC, 但对比度强, 图像清晰的仅为1%。也有一些学者使用高分辨率的MRI进行MIC的检查, 但由于其等待时间长, 成本高, 可用性有限等原因, 使得该项技术并没有得到很好的推广。
CBCT由于其高分辨率, 低辐射剂量, 三维重建图像质量高, 可精确测量, 已成为临床诊治口腔颌面部疾病的重要检查手段[6, 7]。Makris等[8]利用CBCT进行研究, 发现有83.5%的MIC可明确显示。黄弘等[9]通过CBCT检查发现80例患者中, 63例(占78.75%)的CBCT影像上可以观测到MIC影像。Pereira等[10]通过CBCT检查发现100%的CBCT图像上都能观察到MIC。研究结果表明, 所有的MIC都是由颏孔位置开始, 在第一前磨牙对应处100%能观察到MIC, 在尖牙区域也有95%能观察到, 有23%在切牙区仍能观察到。传统观念中我们认为下颌颏下区是一个相对安全的位置, 因为下牙槽神经在颏孔区出来, 在进行切牙区种植手术的时候并不经常考虑种植体的长度。但按照我们的研究结果, 有23%MIC在切牙区仍能观察到。如果种植体过长就有可能接触到切牙区的MIC, 术后就可能出现神经麻木, 血肿等症状。对颏部发育不良的患者, 颏成形术是一个非常有效又简单的手术, 传统观念认为, 在根尖下5 mm, 颏孔前5 mm, 离开下颌下缘5 mm的区域是非常安全的手术区域[11], 但临床上仍有报道在此位置上进行手术后出现麻木, Joshi[12]指出, 最大可能是在手术中损伤了颏神经在下颌切牙区的分支。Kong N等[13]也报道了一例由于在颏部取骨而损伤MIC从而造成患者术后一年仍然感觉疼痛和麻木的病例, 目前也已经有不少医生报道在下颌颏孔间区进行的种植手术, 颏部取骨手术或颏成形术等术后出现神经麻木, 水肿, 骨整合失败等并发症, 推测可能的原因就是在术中损伤了MIC[14]。Pommer等[15]提出最新的颏部取骨的安全范围是在根尖下至少8 mm, 取骨的深度最深为4 mm。
我们对MIC与周围组织的三维关系进行了定量测量, 测量结果表明MIC到颊侧骨板的距离远小于到舌侧骨板的距离, 这提示我们在进行种植体手术时, 应注意植入的角度, 偏向舌侧的角度植入可能会更安全。数据按年龄 分为3组, 3组间的数据均无统计学差异, 有报道指出10~19岁人群的其数据与成人存在显著性差异[9], 这可能和下颌骨未发育完全有关, 有待我们进一步研究。按照性别进行分类, 结果表明MIC与下颌骨下缘的距离在男女中存在统计学差异, 女性MIC更靠近下颌骨下缘, P< 0.05。在进行颏下区手术时, 应提前拍摄CBCT, 测量MIC的大小长度以及与周围组织的距离, 以便在安全的区域内完成手术。
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|